







Virus divides ‘haves’ from ‘have-nots’
By Matthew Nelson
As I work through my day at a Navajo Nation border-town clinic, an initially quiet but certainly present simmer of racism or classism has seemingly come to a boil.
Just one month ago — seemingly a lifetime ago in COVID time — my father who lives and works in the metro New York City area where I grew up, posited that “this disease will really divide the haves from the have nots.”
I recall responding that every disease reveals the unfortunate —though structured — sequellae of poverty.
The Navajo Nation is no exception to both poverty and structural violence, as unemployment, disease, and lack of essential utilities have been a longstanding baseline. Classism and racism get lost in the day-to-day sometimes on the reservation but in border towns, it’s stark and it can be ugly.
For the last month or so, I have been echoing to patients and the community the same message coming from the Navajo Nation suggesting that COVID-19 is gaining traction on the reservation, but without numbers, it’s difficult to conceptualize, so I started tracking it relative to other states.
I figured that given the main body of the reservation is geographically larger than several states and about the size of West Virginia, it should be compared to other states. It should be noted that the relatively small Hopi Reservation resides completely within the borders of the Navajo Nation, and while a different people and culture, are functioning within the same geographic space and being seen by the same health care facilities.
As a public service, the Navajo Times is making all coverage of the coronavirus pandemic fully available on its website. Please support the Times by subscribing.
How to protect yourself and others.
Why masks work. Which masks are best.
Resources for coronavirus assistance
By the end of March, just 15 days from when the first couple of cases were reported on Navajo, there were 116 cases per 100,000 people, taking the third spot among the hardest-hit states at that time. Just 12 days later, on April 11, 2020, the Navajo Nation had 465 cases per 100,000, still only trailing New York state (920) and New Jersey (655).
By the end of April, cases per capita had risen on the Navajo Nation to 1,427, second only to the state of New York, while deaths per capita rank fifth in the United States relative to the states. (https://tinyurl.com/y93jhcqa).
It was not hard to predict that COVID-19 would have success among a people with limited running water, limited electricity, limited telecommunications, housing insecurity, and frank poverty.
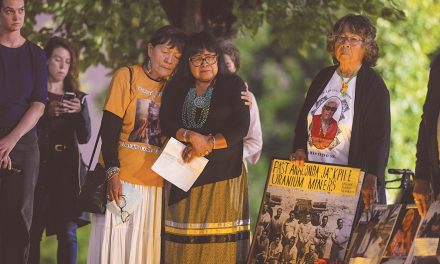
Among the “haves and have nots,” the population of the Navajo Nation would largely be placed in the latter group. Historical and structural violence, characterized by events such as the Long Walk, stock reduction policies, Bennett Freeze, and the underfunding of treaty-bound access to health care, have taken their toll.
Unemployment has always been alarming in this region, upwards of 50 percent prior to COVID. Disease risk has also been starkly different than the rest of the country as American Indians normally see death from diseases such as diabetes at rates three times higher, chronic liver disease 4.5 times higher, assault and homicide two times higher, and death from influenza and pneumonia at a rate two times higher than the United States in general (https://tinyurl.com/y5cfrfsv).
Although several indicators can easily identify the Navajo Nation as a place ripe for morbidity and mortality, over a century of social adaptive responses to a structurally violent baseline have yielded a people with tremendous resilience, ingenuity, resourcefulness, and grace.
Hard work is expected. People build their own homes and are able mechanics. Frugality is an art, manifested most notably in the butchering of a prized family sheep. Language and culture are respected as survival mechanisms, and the elderly are revered, honored and cared for by family turned home health providers.
At work, I generally see a majority Navajo population, several of which are elderly who struggle with diabetes, heart disease, obesity and rheumatoid arthritis among others. I share in the struggles of the clinic staff as we try to flex and bend with the current environment of COVID-19.
While trying to serve patients best, we are also trying to first and foremost, do no harm. We have seen several patients with COVID in our clinic and have been able to re-schedule those who would face potential harm in visiting the clinic. Additionally, we have been able to visit with patients over the phone or via telehealth technology, which has lessened the potential exposure of the staff, allowing us to be more available to serve our community.
We are still testing for COVID in the parking lot, have essentially turned a patient’s car into the new waiting room, started running prescriptions from the pharmacy to a patient’s vehicle, and tried to keep as many non-essential visits to a minimum.
However, over the final week of April, I am noticing a common thread in the disposition of some patients and community members. Where initially, telemedical visits were entertained, more and more patients are now demanding to be seen in person, telling me they feel the COVID crisis is overblown or overhyped by the media, or “the cure is worse than the disease,” or “it’s no worse than the flu.”
Although this is striking to me as a health care provider who has seen the toll, it nonetheless promotes intrigue regarding why a community just a stone’s throw from one of the top two per capita crises in the nation would miss the boat here. How can you see so much death and devastation (complete with a National Guard response) on one hand, and suggest it is overblown on the other?
When this sentiment initially started to persistently pop into my everyday life, I figured it was likely related to a perceived loss of worth that comes from joblessness. Perhaps it was related to social and familial upheaval and displacement. I have seen similar emotions among refugee populations I have worked with the in past (https://tinyurl.com/y87avmzx <https://tinyurl.com/y87av>).
However, by the start of May, I am becoming more concerned that this is not as much a drive to eliminate feelings of worthlessness, but a lack of empathy — an impossibility of empathy, and indeed, the majority of the “overblown” sentiment seemed to anecdotally be from a non-Navajo demographic.
In my telemedical visits with patients on the reservation, they often report to me on their COVID response. Many are living in their even more remote sheep-camp locations. Their lives are completely disrupted by stay-at-home and curfew orders from the Navajo Nation, complete with police checkpoints that will cite citizens if traveling after hours without permission.
Some patients and staff request letters from me to support their safe passage through these checkpoints on the way to work at a health care facility or for essential medical appointments such as prenatal appointments for patients that have been told to go elsewhere for care.
Families without electricity are forced to make trips to town for food that can’t be stored easily. Families are still traveling to town for large containers of water that will be shared among family and livestock, or to pick up medication that can’t be mailed to their homes for lack of physical addresses or postal delivery services. Funerals and mortuary services are now in even higher demand, as single families grieve for multiple family members at once.
So how is this overblown? How is the cure, which is arguably more difficult for Navajo under curfew and stay-at-home orders in the context of poverty, worse than the disease?
I don’t mean to essentialize this to something petty, but I can’t help but ask myself how we can value our “non-essential” economy of restaurants, haircuts, malls, etc., over human lives in our communities?
It reminded me of something I noticed as an anthropology graduate student many years ago while working on the reservation. It is the realization and awful concession that Navajo and brown lives do not take priority over white political, monetary, or other agendas. Protests, both online and in person, suggest that brown lives indeed matter less than haircuts. They matter less than the inconvenience of closures to recreational destinations — albeit a significant economic inconvenience.
As medical providers, it’s difficult to see a population do something that is obviously opposed to their best health interests, but that’s part of the job, so we warn, educate, and work fervently nonetheless.
Re-opening may bring haircuts back for some, but it will surely bring infection and death to many more, particularly the vulnerable, marginalized, and forgotten of this country: black and brown communities, the poor, those incarcerated, and the senior population.
As the state of Utah organized an impressive military demonstration of F-35s in what was supposed to be a thank you to health care providers. It also heralded a transition point for several states to begin opening up businesses again.
I can tell you from the perspective of a health care provider who watches helicopters seemingly constantly fly patients from our critical access hospital to larger facility ICUs for ventilator support, the intended sense of gratitude was not well received.
Although our national curve is flattened, our mission is not accomplished. This is not a time to celebrate and let our guard down. It’s not a time to take a victory lap with F-35s or a stroll through a crowded store.
We still have a virus that has killed tens of thousands more in a single month than flu kills in an entire year that is slowly working its way across the country and will continue to rack up an increasingly impressive death toll, likely to overlap with the flu season a few months away.
We still have shortages of PPE and tests. We still have several thousand more funerals to arrange.
Black and brown communities still suffer disparately, and sure enough, just like all other disease in this country, COVID-19 is easily juxtaposing the “haves” from the “have nots.”
Matthew Nelson is a physician anthropologist in Page, Arizona.
 Highway 264,
Highway 264, I-40, WB @ Winslow
I-40, WB @ Winslow{kind=link}